Hepatitis Viruses Mnemonic
Hepatitis Viruses Mnemonic
P residential H onor F ree D.C.
Virus & Lab
A = P icornavirus, naked capside, RNA, anti-HAV-IgM
B = H epadnavirus, enveloped, DNA, anti-HBc IgM, HBsAg, HBeAg
C = F lavivirus, enveloped, RNA, anti-HVC ELISA
D = D efective, enveloped circular RNA, anti-HDV ELISA
E = C alcivirus, naked capsid, RNA, -

More Posts from T-b-a-blr-blog and Others

It’s Medical Mnemonics Monday!
Renal Papillary Necrosis is a form of nephropathy characterized by coagulative necrosis of the renal medullary pyramids and papillae.
Causes of Papillary Necrosis can be remembered by the mnemonic “POSTCARDS”.
P yelonephritis
O bstruction of the urogenital tract
S ickle cell disease
T uberculosis
Chronic liver disease,
A nalgesia /A lcohol abuse,
R enal transplant rejection
D iabetes mellitus
S ystemic vasculitis
Check out the list of the previous Medical Mnemonics here.
Antimicrobial Agents - Cell wall inhibitors
Based on mode of action • divided into families based on chemical structure
Modes of action Interference with:
cell wall synthesis
protein synthesis
nucleic acid synthesis
plasma membrane integrity
metabolic pathway
Inhibitors of Bacterial Cell Wall (peptidoglycan) Synthesis
The Beta-lactam Family
The Glycopeptides

Peptidoglycan is composed of N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) repeat units, and amino acids. Each NAM is linked to peptide chain and the peptide chains are cross-linked.
β-lactams
Includes penicillin derivatives (penams), cephalosporins (cephems), monobactams, and carbapenems.
class of broad-spectrum antibiotics containing a β-lactam ring
Bacterial transpeptidase enzymes are responsible for catalysing cross-linking of the peptide chains
β-lactam ring bind to these transpeptidases – this inhibits cross-linking between peptide chains and prevents synthesis of stable PG
Cell wall synthesis ceases and the bacterial cells eventually die due to osmotic instability or autolysis.

Glycopeptides
Polypeptide agents - basic structural elements amino acids
Vancomycin:
complexes with peptide portion of peptidoglycan’s precursor units
vancomycin is a large hydrophilic molecule able to form hydrogen bonds with the terminal D-alanyl-D-alanine moieties of the NAM/NAG-peptides
preventing PG transglycosylation reaction – PG precursor subunits (NAG-NAM+peptide) cannot be inserted into peptidoglycan matrix;
Vancomycin also alters bacterial-cell-membrane permeability and RNA synthesis
Uses: serious Gram positive infections e.g. MRSA wound infection
Adverse effects:
damage to auditory nerve
hearing loss (ototoxicity)
“Red man/neck” syndrome - rash on face, neck, upper torso

Tick-Borne Diseases

Endospore
Elek test to document toxi production of Corynobacterium diphteriae
Antibiotics: Protein Synthesis Inhibitors
Protein Synthesis
Formation of Initiation Complex (tRNA in P site)
aa incoorporation (tRNA in A site, aminoacyl-tRNA)
Formation of Peptide Bond (peptidyltransferase)
Translocation

MNEMONIC: “ALi eSTá Cuasi MAL”
* Inhibit 1: “ALi”
A minoglycosides
Li nezolid
* Inhibit 2: “eSTá”
S treptogramins
T etracyclins
* Inhibit 3: “Cuasi”
C loramphenicol
* Inhibit 4: "MAL"
M acrolides
A minoglycosides
L incosamides
Micobacterium tuberculosis DX
Auramine-Rhodamine staining bacilli: fluorescent apple green (sensitive but not specific). If positive, do acid fast.

Acid Fast

Lowenstein-Jensen medium: aerobic, slow growing (2-3weeks)

PPD or Mantoux Test: measure 48-72h after. POSITIVE: >/= 5mm in VIH+ pts, >/=10mm in high risk population (IVDA, poverty, immigrants from high TB area, physicians, nurses), >/=15mm in low risk population

Positive indicates exposure, but not necessarily active disease.
Quantiferon-TB Gold Test: measures IF-gamma

Niacin producers
Catalase negative at 68° and catalase active at body T°
No serodiagnosis




11.19.17
2 more days until break
Music mood: Mili - Miracle Milk

Who wants a box of chocolates when you can have a petri dish of bacteria?
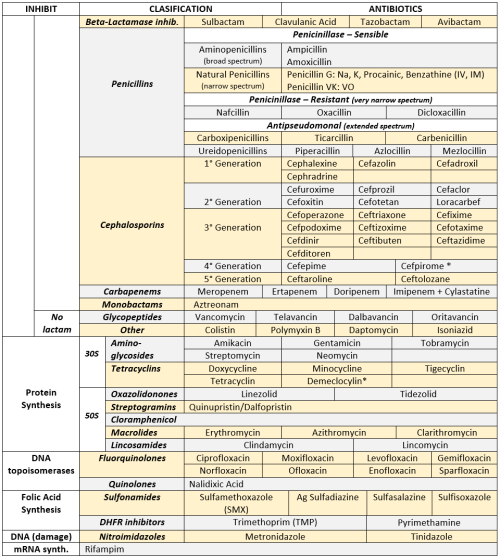
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci

* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines

* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones
-
 theperksofbeingatenneseetee-blog liked this · 2 months ago
theperksofbeingatenneseetee-blog liked this · 2 months ago -
 yesyoushouldbestudying reblogged this · 1 year ago
yesyoushouldbestudying reblogged this · 1 year ago -
 seowens88 liked this · 2 years ago
seowens88 liked this · 2 years ago -
 wiselovecollection-things-blog liked this · 2 years ago
wiselovecollection-things-blog liked this · 2 years ago -
 themidnightmedic liked this · 2 years ago
themidnightmedic liked this · 2 years ago -
 hun4 liked this · 4 years ago
hun4 liked this · 4 years ago -
devinfreetime liked this · 5 years ago
-
 paureus reblogged this · 5 years ago
paureus reblogged this · 5 years ago -
 craftybanditexpertgiant liked this · 6 years ago
craftybanditexpertgiant liked this · 6 years ago -
 t-b-a-blr-blog reblogged this · 6 years ago
t-b-a-blr-blog reblogged this · 6 years ago -
t-b-a-blr-blog liked this · 6 years ago
-
jayvadodariya liked this · 7 years ago
-
 nukeeeeeeeeeee-blog reblogged this · 7 years ago
nukeeeeeeeeeee-blog reblogged this · 7 years ago -
drart90 reblogged this · 7 years ago
-
 imsorryicouldntgivemoreblr liked this · 7 years ago
imsorryicouldntgivemoreblr liked this · 7 years ago -
 mona96us liked this · 8 years ago
mona96us liked this · 8 years ago -
 erotik-seniorentreff-wien liked this · 8 years ago
erotik-seniorentreff-wien liked this · 8 years ago -
 sofiajamilb-blog liked this · 8 years ago
sofiajamilb-blog liked this · 8 years ago -
brynaert-a-blog liked this · 8 years ago
-
 aemun50-blog reblogged this · 8 years ago
aemun50-blog reblogged this · 8 years ago -
aemun50-blog reblogged this · 8 years ago
-
 bubblewrapmyself liked this · 8 years ago
bubblewrapmyself liked this · 8 years ago -
 chao-ab-ordo liked this · 8 years ago
chao-ab-ordo liked this · 8 years ago -
 jagoayeea liked this · 8 years ago
jagoayeea liked this · 8 years ago -
doctor2019 liked this · 9 years ago
-
 charminglynne reblogged this · 9 years ago
charminglynne reblogged this · 9 years ago -
charminglynne liked this · 9 years ago
-
nekomed-blog liked this · 9 years ago
-
 singledose reblogged this · 10 years ago
singledose reblogged this · 10 years ago -
 londondreaming11 liked this · 10 years ago
londondreaming11 liked this · 10 years ago -
 inoshie reblogged this · 10 years ago
inoshie reblogged this · 10 years ago -
inoshie liked this · 10 years ago
-
 pre-med-timelord reblogged this · 10 years ago
pre-med-timelord reblogged this · 10 years ago -
 40milesfromthesun reblogged this · 10 years ago
40milesfromthesun reblogged this · 10 years ago -
40milesfromthesun liked this · 10 years ago
-
 drcaro-ccm liked this · 10 years ago
drcaro-ccm liked this · 10 years ago -
drcaro-ccm reblogged this · 10 years ago
-
 andimedicine reblogged this · 10 years ago
andimedicine reblogged this · 10 years ago -
 jfk33 liked this · 10 years ago
jfk33 liked this · 10 years ago -
 thebrunettedoc reblogged this · 10 years ago
thebrunettedoc reblogged this · 10 years ago -
 maricela1289 reblogged this · 11 years ago
maricela1289 reblogged this · 11 years ago
