
195 posts
Latest Posts by t-b-a-blr-blog - Page 5







Immuno
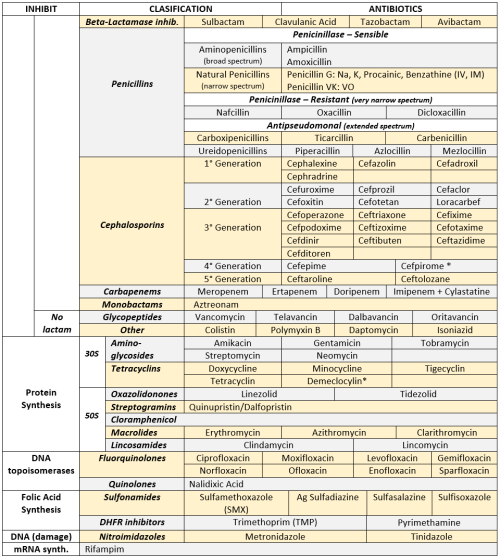
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci

* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines

* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones

Bacteria and fungi in petri dishes
Klari Reis uses plastics, paints and other mediums to create the idea of bacteria and biological matter within petri dishes




05-11-18 bio notes! i tried out a new background and i think it looks really pretty!! i hope you guys like it :). i had my first test for my dissection lab and my group ended up getting 100%! the next few tests are harder, but i think we’ll all do gr8. i hope you all had a great week!

Different anatomy notes form this semester Supplies used (not all at once, I mix and match): Faber-Castell Coloured Pencils (48 Pack) - https://amzn.to/2Kd1mUy Staedtler Triplus Fineliners - http://amzn.to/2pghonI Stabilo Point 88 Fineliner - https://amzn.to/2qU8fC9 Sharpie Pens - https://amzn.to/2HTRmP2 Uni Pin 0.1 Fineliner - https://amzn.to/2HmXp1z Crayola Supertips - https://amzn.to/2HVW1jr Bic Ballpoint Pen - https://amzn.to/2HmCjk0 Stabilo Swing Cool Highlighters - https://amzn.to/2HKxPTu

This bedroom is soooo pretty, this colour palette is everything.



Tumblr room🌹



Pizza heaven! Quick and easy! Recipe up on blog: www.studydiaryofamedstudent.wordpress.com


New background! Download higher quality photo here!
https://drive.google.com/file/d/1F5SlJmB8YiNNtGuKrc-QtMnrrjZ1tOHL/view?usp=sharing
April Background

I created this new background for April! A reminder to all the great girls out there who are awesome human beings!

For a high quality foto, check out the link in my previous post!


20.1.18 // studygram: alimastudies
i don’t normally upload pictures of my homework because i don’t tend to spend a lot of effort or time on them as i know i won’t be using it again, but for this biology homework i thought i would do it nicely and use it for my future notes! i need to work on my handlettering oh dear god ahhh i used a crayola supertip for it
be patient, good things are coming your way :)

Me this week

Motivation can be experienced differently for each of us. While some people just get this kind of impulsive motivation, others develop their motivation through actions.
@masterposts @studymasterposts
I would like to show you why it is wrong to wait for your motivation and why you should just do something instead - it doesn’t matter how big your action is.
How to gain motivation
OK, so just like I told you above there exists a concept of just doing some random shit. That means that you start small even though you know that you should do more.
You need to write an essay in two days but you’re spending all the time watching a cat jumping from a window? (if you followed the link - yeah, it’s funny but please continue reading my bullshit lol)
The solution to your stressful task is to start doing something even if it doesn’t seem big or challenging. (In our example with the essay this would mean, starting the writing program/ writing “Outline for my essay” on a paper/ starting a draft as small as possible etc.)
You need to clean your room? Search the smallest task and do this one: put your old pizza that’s laying on the floor in the trash can and your underwear where it belongs - you don’t want your dog to eat it, right?
You want to get fit and start working out? Maybe you had an impulse of motivation one week ago, but now you’re laying on the couch like the cutest panda ever, eating sweets and asking yourself where your motivation went.
You already have an idea what you need to do now, right? Just do one push-up/ lunge/ crunch whatever.
It doesn’t matter how small your action is, but if you experience the feeling of this small success you’ll keep going.
How to stay motivated (Part 1)
Now that you’re finally motivated (doesn’t matter how), you really need to stick on that workflow or whatever you’re trying to achieve. One of the simplest things to maintain your motivation is to think of why you started. Here are some examples:
I know that I’m able to get this shit done.
I want to prove that I can do more than I thought.
I want to show everybody that I’m taking my responsibilities seriously.
I need to pass that exam.
Failing is worse than studying.
etc. (the reason needs to come from your heart - if it isn’t true, it won’t work)
Another way (which is pretty simple and works pretty good for most of the people) is the chain system:
Draw 31 boxes (for one month) and tick one each day after completing your task. This method is pretty common because it is pretty simple and works for no matter how much time you want to do your habit. (The lovely @emmastudies has created a lot of wonderful printables, maybe you find more details there for study tracking.) After keeping up with the growing chain, you’ll be thinking twice before interrupting the chain and stopping your chain.
Part 2 will be posted on Friday, 06.01.
Innate Immunity - intro
First line of defence + first to act
A primitive response (exists in animals and some plants)
Non-specialised and without ‘memory’
Consists of:
Physical barriers (eg skin and mucosa//tight junctions, airflow)
Chemical barriers (eg enzymes, lung surfactant, antimicrobals)
Soluble mediators of inflammation (eg cytokines)
Microbal defence (eg commensal competition, secreted antimicrobals)
Cells (eg phagocytes)
Receptors to recognise presence of pathogen/injury - results in inflammation

Soluble Mediators
Complement Proteins
liver-derived
circulate in serum in inactive form
activated by pathogens during innate response
functions include lysis, chemotaxis and opsonisation

Auxiliary Cells
Mediate inflammation as part of the immune response. The main auxiliary cells involved in the immune response are Basophils, Mast cells and Platelets.
Basophils
Leukocyte containing granules
on degranulation release histamine + platelet activating factor
causing increased vascular permeability and smooth muscle contraction
also synthesise and secrete other mediators that control the development of immune system reactions
Mast Cells
Also contain granules
However they are not circulating cells - found close to blood vessels in all types of tissue especially mucosal and epithelial tissues.
rapidly release inflammatory histamine but this is IgE dependant so not innate
Platelets
normally function in blood clotting
also release inflammatory mediators

Cytokines and chemokines
Produced by many cells but especially mØ (macrophages), initiate inflammatory response and act on blood vessels
interferons - antiviral protection
chemokines - recruit cells
interleukines - fever inducing, IL-6 induces acute phase proteins
IL-1 - encourages leukocytes to migrate to infected/damaged tissue
as does tumour necrosis factor (TNFa)
Acute phase proteins
Liver derived proteins
plasma concentrations increase (positive acute-phase proteins) or decrease (negative acute-phase proteins) in response to inflammation
called the acute-phase reaction
triggered by inflammatory cytokines ( IL-1, IL-6, TNFα)
help mediate inflammation ( fever, leukocytosis, increased cortisol, decreased thyroxine, decreased serum iron, etc)
activate complement opsonisation
Inflammation

Cells
Cytotoxic Cells
Eosinophils/natural killer cells, cytotoxic T cells
kill target via release of toxic granules
dendritic cell derived IL-12 helps activate NK cells
Phagocytes
mono-nuclear = long-lived; polynuclear = short-lived
engulf, internalize and destroy
phagosome forms around microbe
enzyme filled with lysosomes fuses to form phagolysosome
organism is digested
fragments are either ‘presented’ or exocytosed

phagocytosis requires recognition of microbe via receptors for
PAMPs (pathogen associated molecular patterns - eg flagella or capsule) - recognised by toll-like receptors
activated complement
antibody
The innate immune response primes for the adaptive
B-cells are primed by activated complement
Th1 cell differentiation needs pro-inflammatory cytokines
Passive Immunotherapy
Active immunotherapies:
Cytokines (TNFa IL-2, IFNs)
Cancer vaccines
tumour CTL and APC
DC priming
Passive immunotherapy:
Administration of monocolnal (clone derived asexually from a single individual or cell) antibodies which target either tumour-specific or over expressed antigens
Generally comprised of antibodies made outside of the body (in a lab)
administered to patients to provide immunity against a disease, or to help fight existing disease
do not stimulate a patient’s body to ‘actively’ respond to a disease the way a vaccine does
immunogen is given several times to induce a strong secondary response
blood serum contains many different antibodies to the immunogen
most immunogens have multiple antigenic epitopes
each stimulates a different B cell clone/receptor –> polyclonal antibody (PAb) response

Monoclonal antibody (mAb) therapy is the most widely used form of cancer immunotherapy. Monoclonal antibodies cannot be purified from a polyclonal sample and are derived from a single clone/specific for a single epitope.

Antibodies in cancer therapy:
Trigger immune system to attack cancer cells
Block molecules that stop the immune system working (checkpoint inhibitors)
Block signals telling cancer cells to divide
Carry drugs or radiation to cancer cells
Checkpoint inhibitors
Immune system uses particular molecules to stop it being over activated and damaging healthy cells - these are known as checkpoints
some cancers make high levels of checkpoint molecules to switch of immune system T cells which would normally attack cancer cells
examples of targets include CTLA-4, PD-1 and PD-L1 (programmed death ligand 1)

Blocking cell division signals
Cancer cells often express large amounts of growth factor receptors on their surface –> rapid cell division when growth factors stimulate them
some monoclonal antibodies stop growth factor receptors working
either by blocking the signal or the receptor itself
cancer no longer gets signal to divide

Carrying drugs/radiation
drugs or radioisotopes can be attached to monoclonal antibodies
the mAB binds to the cancer cell, delivering directly
known as conjugated MABs

Antibodies (Human)

The ‘foot’ (bottom) of the antibody is known as the Fc fragment - binds to cells, binds to complement = effector function (kills or removes antigen)
The top (antigen binding) is the Fab fragment
Chains are held together with disulphide binds
Associated molecules allow intracellular signalling
Normally 3X constant heavy chain domains per chain and a hinge region (except μ and ε which have 4 and no hinge region)
Classes of Immunoglobulins
The five primary classes of immunoglobulins are IgG, IgM, IgA, IgD and IgE, distinguished by the type of heavy chain found in the molecule.
IgG - gamma-chains
IgMs - mu-chains
IgAs - alpha-chains
IgEs - epsilon-chains
IgDs - delta-chains.
Differences in heavy chain polypeptides allow different types of immune responses. The differences are found primarily in the Fc fragment. There are only two main types of light chains: kappa (κ) and lambda (λ), and any antibody can have any combination of these 2 (variation).
IgG
monomer
Gamma chains
70-85% of Ig in human serum.
secondary immune response
only class that can cross the placenta - protection of the newborn during first 6 months of life
principle antibody used in immunological research and clinical diagnostics
21 day half life
Hinge region (allows it to make Y and T shapes - increasing chance of being able to bind to more than one site)
Fc strongly binds to Fcγ receptor on phagocyte - opsono-phagocytosis
Activates complement pathway

IgM
Serum = pentamer
Primary immune responses - first Ig to be synthesised
complement fixing
10% of serum Ig
also expressed on the plasma membrane of B lymphocytes as a monomer - B cell antigen receptor
H chains each contain an additional hydrophobic domain for anchoring in the membrane
Monomers are bound together by disulfide bonds and a joining (J) chain.
Each of the five monomers = two light chains (either kappa or lambda) and two mu heavy chains.
heavy chain = one variable and four constant regions (no hinge region)
can cause cell agglutination as a result of recognition of epitopes on invading microorganisms. This antibody-antigen immune complex is then destroyed by complement fixation or receptor mediated endocytosis by macrophages.
In humans there are four subclasses of IgG: IgG1, IgG2, IgG3 and IgG4. IgG1 and IgG3 activate complement.

IgD
B cell receptor
<1% of blood serum Ig
has tail pieces that anchor it across B cell membrane
forms an antigen specific receptor on mature B cells - consequently has no known effector function (don’t kill antigens, purely a receptor) (IgM as a monomer can also do this)

IgE
Extra rigid central domain
has the most carbohydrates
IgE primarily defends against parasitic invasion and is responsible for allergic reactions.
basophils and tissue mast cells express very high affinity Fc receptors for IgE - mast cells then release histamine
so high that almost all IgE is bound
sensitizes (activates) mucosal cells and tissues
protects against helminth parasites
IgE’s main purpose is to protect against parasites but due to improved sanitation these are no longer a prevalent issue across most of the world. Consequently it is thought that they become over activated and over sensitive while looking for parasites and start reacting to eg pollen and causing allergies.

IgA
Exists in serum in both monomeric (IgA1) and dimeric (IgA2) forms (dimeric when 2 Fcs bind via secretory complex)
15% of the total serum Ig.
4-7 day half life
Secretory IgA2 (dimer) = primary defense against some local infections
Secreted as a dimer in mucous (e.g., saliva, tears)
prevents passage of foreign substances into the circulatory system


Isotype: class of antibody (IgD, IgM etc)
Allotype: person specific alleles
Idiotype: (hyper) variable region - antibody specificity
Leukocyes (WBCs) & Defence
A summary
Neutrophils - non-specific defence against bacteria and fungi
Eosinophils -Defence against parasites; dampen allergic response
Basophils - Anaphylactic & inflammation response
Monocytes - Mature into macrophages, engulf foreign substances; remove aged RBCs and other debris
Lymphocyes - Recognise antigens, various roles
Haematology
White Blood Cells (Leukocytes)

Neutrophils, eosinophils and basophils = granulocytes (polymorphonuclear leukocytes)
Monocytes & lymphocyes = mononuclear
Neutrophils
Most numerous (~60% of WBC)
Nucleus divided into lobes
Cytoplasm contains small granules
Stains pink with Romanowsky dyes
Lifespan of 6-10hrs
Exit into tissues - non-specific defence against bacteria and fungi

Eosinophils
1% of circulating leukocytes
Large cytoplasmic granules - stain strongly with acidic dye eosin
Nucleus is bilobed
Circulate for 4-5hrs
Exit to tissues –>
Defence against parasites
Dampen allergic response
Tissue eosinophils are also capable of responding to bacterial and fungal infection in a similar way to neutrophils.

Basophils
Least numerous (<1%)
Large granules stain strongly with basic dye methylene blue
Involved in anaphylactic hypersensitivity and inflammatory reactions

Monocytes
5% of circulating leukocytes
Large cell
Kidney/clefted shaped nucleus
Scattering of delicate azurophilic granules
Circulate for 10hrs
Mature into phagocytic tissue macrophages
Responsible for the removal of aged RBCs and other debris
Process and present antigens to T-lymphocytes

(Macrophages are formed in response to an infection or accumulating damaged or dead cells. Large, specialized cells that recognize, engulf and destroy target cells.)

Lymphocytes
Second most common leukocyte (33%)
Much less cytoplasm - nucleus almost fills cell
Variable lifespan
Receptors on surface recognise foreign substances

Several types of lymphocyte - click here
Archaea
Archaeans are single-celled and join bacteria to make up the Prokaryotes. The Archaea classification is a very recent discovery, due to the similarities in appearance and behaviour to bacteria they weren’t separated until the late 1970′s. They mostly live in extreme environments and can be sub grouped:
Methanogens - produce methane gas as a waste product of their “digestion,” or process of making energy.
Halophiles - live in salty environments.
Thermophiles - live at extremely hot temperatures.
Psychrophiles — those that live at unusually cold temperatures.
Like bacteria, archaea lack a true nucleus. Both bacteria and archaea usually have one DNA molecule suspended in the cell’s cytoplasm contained within a cell membrane. Most, but not all, have a tough, rigid outer cell wall.

use a variety of substances for energy, including hydrogen gas, carbon dioxide and sulfur.
many archaea thrive in conditions mimicking those found more than 3.5 billion years ago. [eg oceans that regularly reached boiling point — an extreme condition not unlike the hydrothermal vents and sulfuric waters where archaea are found today]
Antimicrobial Agents - Cell wall inhibitors
Based on mode of action • divided into families based on chemical structure
Modes of action Interference with:
cell wall synthesis
protein synthesis
nucleic acid synthesis
plasma membrane integrity
metabolic pathway
Inhibitors of Bacterial Cell Wall (peptidoglycan) Synthesis
The Beta-lactam Family
The Glycopeptides

Peptidoglycan is composed of N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) repeat units, and amino acids. Each NAM is linked to peptide chain and the peptide chains are cross-linked.
β-lactams
Includes penicillin derivatives (penams), cephalosporins (cephems), monobactams, and carbapenems.
class of broad-spectrum antibiotics containing a β-lactam ring
Bacterial transpeptidase enzymes are responsible for catalysing cross-linking of the peptide chains
β-lactam ring bind to these transpeptidases – this inhibits cross-linking between peptide chains and prevents synthesis of stable PG
Cell wall synthesis ceases and the bacterial cells eventually die due to osmotic instability or autolysis.

Glycopeptides
Polypeptide agents - basic structural elements amino acids
Vancomycin:
complexes with peptide portion of peptidoglycan’s precursor units
vancomycin is a large hydrophilic molecule able to form hydrogen bonds with the terminal D-alanyl-D-alanine moieties of the NAM/NAG-peptides
preventing PG transglycosylation reaction – PG precursor subunits (NAG-NAM+peptide) cannot be inserted into peptidoglycan matrix;
Vancomycin also alters bacterial-cell-membrane permeability and RNA synthesis
Uses: serious Gram positive infections e.g. MRSA wound infection
Adverse effects:
damage to auditory nerve
hearing loss (ototoxicity)
“Red man/neck” syndrome - rash on face, neck, upper torso
Antimicrobial Agents - Inhibition of DNA and Protein Synthesis
Bacterial chromosome replication

DNA replication

Bacterial Topoisomerases
maintain DNA in appropriate state of supercoiling
cut and reseal DNA
DNA gyrase (topoisomerase II) introduces negative supercoils
Topoisomerase IV decatenates circular chromosomes
these are the targets of the quinolone antibacterial agents
Quinolones
bind to bacterial DNA gyrase and topoisomerase IV after DNA strand breakage
prevent resealing of DNA
disrupt DNA replication and repair
bactericidal (kill bacteria)
Fluoroquinolone is particularly useful against
Gram +ves: Staphylococcus aureus, streptococci
Gram -ves: Enterobacteriacea; Pseudomonas aeruginosa
Anaerobes: e.g. Bacteroides fragilis
many applications e.g. UTIs, prostatitis, gastroenteritis, STIs
Adverse effects
Relatively well tolerated
GI upset in ~ 5% of patients
allergic reactions (rash, photosensitivity) in 1 - 2% of patients

Inhibition of Bacterial Protein Synthesis
Macrolides
in 1952: Erythromycin was isolated as the first macrolide (Streptomyces erythreus)
Newer macrolides: clarithromycin, azithromycin
Structurally they consist of a lactone ring (14- to 16-membered) + two attached deoxy sugars
Mode of action
bind reversibly to bacterial 50S ribosomal subunit
causes growing peptide chain to dissociate from ribosome → inhibiting protein synthesis
bacteriostatic (stops reproduction)

Macrolides’ spectrum of activity
good antistaphylococcal and antistreptococcal activity
treatment of respiratory & soft tissue infections and sensitive intracellular pathogens • e.g. Chlamydia, Legionella
Adverse effects
Generally well tolerated
nausea
vomiting
diarrhoea
rash
Aminoglycosides
large family of antibiotics produced by various species of Streptomyces (“mycin”) and Micromonospora (“micin”)
include: streptomycin, neomycin, kanamycin, gentamicins, tobramycin
Structure = linked ring system composed of aminosugars and an aminosubstituted cyclic polyalcohol
Mode of action of aminoglycosides
Bind irreversibly to 30S ribosomal subunit
disrupt elongation of nascent peptide chain
translational inaccuracy → defective proteins
bactericidal

Spectrum of activity
broad spectrum; mainly aerobic G-ve bacilli (e.g. P. aeruginosa)
used to treat serious nosocomial infections (hospital acquired infections)
First TB antibiotic
Used for cystic fibrosis
Adverse effects
all aminoglycosides have low Therapeutic Index (only a small amount needed to become toxic)
renal damage, ototoxicity, loss of balance, nausea
Cryptosporidium
Cryptosporidium is a microscopic parasite that causes the diarrhoeal disease cryptosporidiosis. Both the parasite and the disease are commonly known as “Crypto.”
The parasite is protected by an outer shell (oocyst)
Allows survival outside the body for long periods of time
Very tolerant to chlorine disinfection.
Water is the most common form of spread
Poses serious risk to immunocompromised individuals, eg AIDS; cancer and transplant patients who are taking certain immunosuppressive drugs.

Symptoms
Symptoms of cryptosporidiosis generally begin 2 to 10 days (average 7 days) after infection.
Watery diarrhea
Stomach cramps or pain
Dehydration
Nausea
Vomiting
Fever
Weight loss
Some people with Crypto will have no symptoms at all.
Symptoms usually last about 1 to 2 weeks (with a range of a few days to 4 or more weeks) in persons with healthy immune systems. Occasionally, people may experience a recurrence of symptoms after a brief period of recovery before the illness ends. Symptoms can come and go for up to 30 days.
In immunocompromised persons Cryptosporidium infections could possibly affect other areas of the digestive tract or the respiratory tract.
Diagnosis & Detection

Cryptosporidium oocysts in a modified acid-fast stain. (CDC Photo; DPDx)
Examination of stool samples.
Detection can be difficult - several stool samples over several days.
acid-fast staining, direct fluorescent antibody [DFA] , and/or enzyme immunoassays
Molecular methods (e.g., polymerase chain reaction – PCR) are increasingly used in reference diagnostic labs,
Treatment
Most people who have healthy immune systems will recover without treatment. Young children and pregnant women may be more susceptible to dehydration resulting from diarrhoea.
For those persons with AIDS, anti-retroviral therapy (improves the immune status) will also decrease or eliminate symptoms of cryptosporidiosis. However, even if symptoms disappear, cryptosporidiosis is often not curable and the symptoms may return if the immune status worsens.
Cryptosporidium and AIDS
Advanced immunosuppression — typically CD4 T lymphocyte cell (CD4) counts of <100 cells/µL — is associated with the greatest risk for prolonged, severe, or extraintestinal cryptosporidiosis.
The three species that most commonly infect humans are Cryptosporidium hominis, Cryptosporidium parvum, and Cryptosporidium meleagridis. Infections are usually caused by one species, but a mixed infection is possible.
Up to 74% of diarrhoea stools in AIDS patients demonstrating the organism in less developed countries where potent antiretroviral therapy is not widely available,
cryptosporidiosis has decreased and occurs at an incidence of <1 case per 1000 person-years in patients with AIDS.4 Infection occurs through ingestion of Cryptosporidium oocysts. Viable oocysts in feces can be transmitted directly through contact with infected humans or animals, particularly those with diarrhea. Oocysts can contaminate recreational water sources such as swimming pools and lakes, and public water supplies and may persist despite standard chlorination (see Appendix: Food and Water-Related Exposures). Person-to-person transmission is common, especially among sexually active men who have sex with men.
Fever is present in approximately one-third of patients and malabsorption is common.
The epithelium of the biliary tract and the pancreatic duct can be infected with Cryptosporidium, leading to sclerosing cholangitis and to pancreatitis secondary to papillary stenosis,
Pulmonary infections also have been reported, and may be under-recognized.
Treatment
ART with immune restoration to a CD4 count >100 cells/µL usually leads to resolution
Treatment of diarrhoea with anti-motility agents (AIII) may be necessary.
Patients with biliary tract involvement may require endoscopic retrograde choledocoduodenoscopy for diagnosis.
Immune reconstitution inflammatory syndrome (IRIS) has not been described in association with treatment of cryptosporidiosis.
No pharmacologic interventions are known to be effective in preventing the recurrence of cryptosporidiosis.
No therapy has been shown to be effective without ART.
Penicillin

Penicillin is a widely used antibiotic prescribed to treat staphylococci and streptococci bacterial infections.
beta-lactam family
Gram-positive bacteria = thick cell walls containing high levels of peptidoglycan
gram-negative bacteria = thinner cell walls with low levels of peptidoglycan and surrounded by a lipopolysaccharide (LPS) layer that prevents antibiotic entry
penicillin is most effective against gram-positive bacteria where DD-transpeptidase activity is highest.
Examples of penicillins include:
amoxicillin
ampicillin
bacampicillin
oxacillin
penicillin
Mechanism(s)
Penicillin inhibits the bacterial enzyme transpeptidase, responsible for catalysing the final peptidoglycan crosslinking stage of bacterial cell wall synthesis.
Cells wall is weakened and cells swell as water enters and then burst (lysis)
Becomes permanently covalently bonded to the enzymes’s active site (irreversible)


Alternative theory: penicillin mimics D-Ala D-Ala

Or may act as an umbrella inhibitor

Resistance
production of beta-lactamase - destroys the beta-lactam ring of penicillin and makes it ineffective (eg Staphylococcus aureus - most are now resistant)
In response, synthetic penicillin that is resistant to beta-lactamase is in use including egdicloxacillin, oxacillin, nafcillin, and methicillin.
Some is resistant to methicillin - methicillin-resistant Staphylococcus aureus (MRSA).
Demonstrating blanket resistance to all beta-lactam antibiotics -extremely serious health risk.
Influenza
Happy flu season! I’ve just been stuck inside for 5 days with a mild case, so this is a bit bitter
There are 3–5 million cases of flu per year, and ~375,000 deaths, usually in older, younger, and immunocompromised individuals.
Enveloped, Single-stranded RNA virus
First identified in 1933, but existed long before
Generally considered an infection of the bronchi
so effectively a form of bronchitis – i.e. it causes inflammation of the bronchi
There are 3 types - A, B and C
B & C appear restricted to humans
C is less common
A is found in wide range of species including pigs and poultry as well as man
Type A appears to be responsible for more severe disease

Basics
Transmission by aerosols
Incubation ~2 days
Contagious during first 3-5days of illness
Symptoms – fever, myalgia, headache, dry cough, sore throat, aches, fatigue
Recovery ~7-10 days for most
Complications – most frequent = secondary bacterial pneumonia, rarely = viral pneumonia, myocarditis, encephalitis
No specific treatment
Vaccination for high risk groups including the elderly, health care workers, those with underlying respiratory conditions.
Avian
The main reservoir is wildfowl that are resistant to the disease
doesn’t usually affect animals other than poultry and pigs
However some transfer events occur
Seasonal
Incidence highest in winter
Strains vary from year to year - hard to predict and vaccinate (this year’s vaccine has been pretty rubbish)
Pandemic
Can be caused by any strain that has not been seen in the human population for many years
New strains evade the herd immunity that exists to previously encountered strains
1918 /19 –( Spanish) estimated 40-50 million deaths worldwide
1957 – Influenza A/H1N1 (Asian)
1968 – Influenza A/H3N2 (Hong Kong)
Eventually the virus runs out of susceptible hosts and the epidemic fizzles out
Experts generally agree another pandemic is inevitable, and may be imminent – maybe we have had some minor pandemics
16000 confirmed H1N1 deaths in 2009 affecting over 200 countries
Consensus is that the prompt action of the Hong Kong authorities probably prevented a pandemic in 1997
The prediction is scary - for industrialised countries they predic 1.0 – 2.3 million hospitalisations
280,000-650,000 deaths
in two years
A network of 112 centres monitor flu isolates to identify unusual strains that can then be examined further
The WHO has a Pandemic Preparedness Plan in place http://www.who.int/influenza/preparedness/pandemic/en/
Diagnosis
Generally based on GP diagnosis
Virus isolation / virus demonstration from nasopharyngeal secretions during acute phase
Demonstration of viral antigen in secretions
Antibody rise using paired sera ( 1st sample taken between days 1-3 of illness, 2nd taken around day 12 of illness) by haemagglutination inhibition or complement fixation test
Molecular methods evolving rapidly – in particular in response to the recent epidemic/pandemic strains emerging
A range of respiratory illnesses have the same symptoms, only laboratory testing can confirm the aetiological agent
Treatment/Vaccination
In the UK NICE argue that immunisation against predicted strains is the best form of defence – traditionally focused on the elderly and those with underlying lung problems, but recently started rolling out a childhood vaccine (nasal spray)
Vaccines generally based on the H & N surface structures which mutate, however hopes of an M protein based vaccine which will give longer lasting protection raised recently
Antivirals
Antivirals not recommended in otherwise healthy people (amantadine should not be used at all) - should ride it out
However when incidence reaches a certain level zanamivir and oseltamivir should be used in those considered high risk for the development of complications – PROVIDED THAT TREATMENT IS STARTED WITHIN 48 HOURS OF ONSET OF SYMPTOMS
Resistance is becoming an issue